
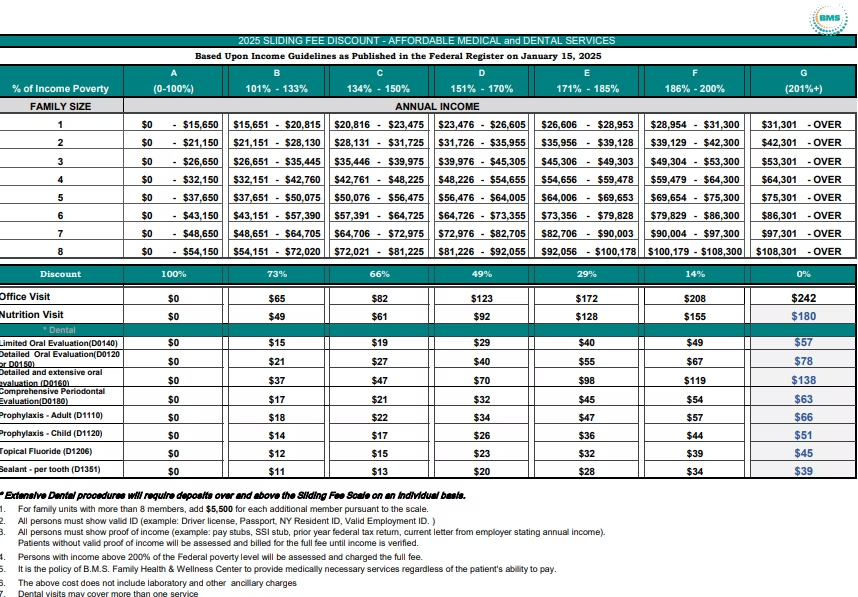
2025 SLIDING FEE DISCOUNT - AFFORDABLE MEDICAL and DENTAL SERVICES
Based Upon Income Guidelines as Published in the Federal Register on January 15, 2025
| FAMILY SIZE | A (0-100%) |
B 101% - 133% |
C 134% - 150% |
D 151% - 170% |
E 171% - 185% |
F 186% - 200% |
G (201%+) |
|---|---|---|---|---|---|---|---|
| % of Income Poverty | (0-100%) | 101% - 133% | 134% - 150% | 151% - 170% | 171% - 185% | 186% - 200% | (201%+) |
| 1 | $0 - $15,650 | $15,651 - $20,815 | $20,816 - $23,475 | $23,476 - $26,605 | $26,606 - $28,953 | $28,954 - $31,300 | $31,301 - OVER |
| 2 | $0 - $21,150 | $21,151 - $28,130 | $28,131 - $31,725 | $31,726 - $35,955 | $35,956 - $39,128 | $39,129 - $42,300 | $42,301 - OVER |
| 3 | $0 - $26,650 | $26,651 - $35,445 | $35,446 - $39,975 | $39,976 - $45,305 | $45,306 - $49,303 | $49,304 - $53,300 | $53,301 - OVER |
| 4 | $0 - $32,150 | $32,151 - $42,760 | $42,761 - $48,225 | $48,226 - $54,655 | $54,656 - $59,478 | $59,479 - $64,300 | $64,301 - OVER |
| 5 | $0 - $37,650 | $37,651 - $50,075 | $50,076 - $56,475 | $56,476 - $64,005 | $64,006 - $69,653 | $69,654 - $75,300 | $75,301 - OVER |
| 6 | $0 - $43,150 | $43,151 - $57,390 | $57,391 - $64,725 | $64,726 - $73,355 | $73,356 - $79,828 | $79,829 - $86,300 | $86,301 - OVER |
| 7 | $0 - $48,650 | $48,651 - $64,705 | $64,706 - $72,975 | $72,976 - $82,705 | $82,706 - $90,003 | $90,004 - $97,300 | $97,301 - OVER |
| 8 | $0 - $54,150 | $54,151 - $72,020 | $72,021 - $81,225 | $81,226 - $92,055 | $92,056 - $100,178 | $100,179 - $108,300 | $108,301 - OVER |
| Discount | 100% | 73% | 66% | 49% | 29% | 14% | 0% |
| Service Type | A | B | C | D | E | F | G |
|---|---|---|---|---|---|---|---|
| Office Visit | $0 | $65 | $82 | $123 | $172 | $208 | $242 |
| Nutrition Visit | $0 | $49 | $61 | $92 | $128 | $155 | $180 |
| Limited Oral Evaluation(D0140) | $0 | $15 | $19 | $29 | $40 | $49 | $57 |
| Detailed Oral Evaluation(D0120) | $0 | $21 | $27 | $40 | $55 | $67 | $78 |
| Detailed and extensive oral evaluation (D0160) | $0 | $37 | $47 | $70 | $98 | $119 | $138 |
| Comprehensive Periodontal Evaluation(D0180) | $0 | $17 | $21 | $32 | $45 | $54 | $63 |
| Prophylaxis - Adult (D1110) | $0 | $18 | $22 | $34 | $47 | $57 | $66 |
| Prophylaxis - Child (D1120) | $0 | $14 | $17 | $26 | $36 | $44 | $51 |
| Topical Fluoride (D1206) | $0 | $12 | $15 | $23 | $32 | $39 | $45 |
| Sealant - per tooth (D1351) | $0 | $11 | $13 | $20 | $28 | $34 | $39 |
* Extensive Dental procedures will require deposits over and above the Sliding Fee Scale on an individual basis.
- For family units with more than 8 members, add $5,500 for each additional member pursuant to the scale.
- All persons must show valid ID (example: Driver license, Passport, NY Resident ID, Valid Employment Card, etc.)
- All persons must show proof of income (examples are: Most recent tax returns, Pay stubs (3 most recent), Letter from employer stating annual income).
- Patients without valid proof of income will be assessed and billed for the full fee until income is verified.
- Persons with income above 200% of the Federal poverty level will be assessed and charged the full fee.
- It is the policy of B.M.S. Family Health & Wellness Center to provide medically necessary services regardless of the patient's ability to pay.
- The above scale does not include laboratory and other ancillary charges.
- Dental visits may cover more than one service.











































{kind=link}
{kind=link}